Tele-operated echograph - Results and Conclusion
Results
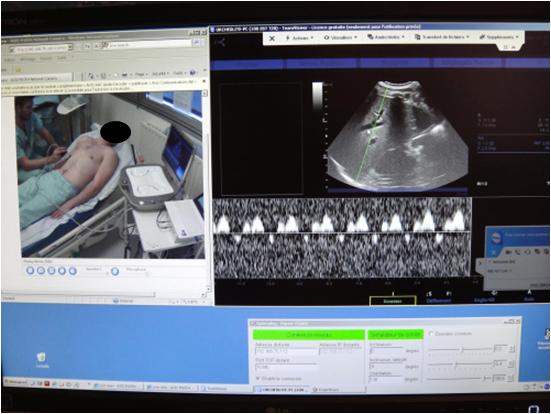
Figure 6 A
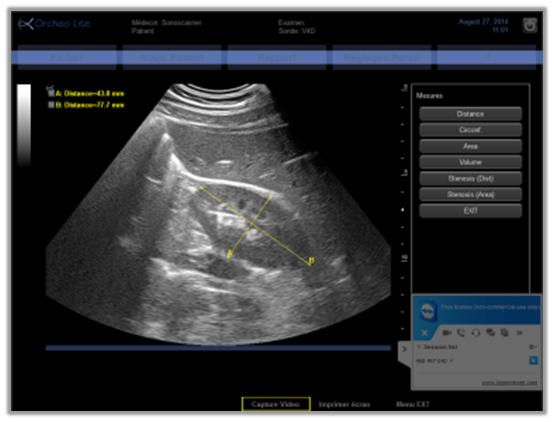
Figure 6 B

Figure 6 C
All examinations were standardized to include imaging and measurements of similar organs and structures. The abdominal examination included B-mode visualization of the pancreas, liver, biliary tract, gall bladder, and the right and left kidneys (Figure 6A and 6B). Pelvic examinations involved the visualization of the bladder, uterus and ovaries, or prostate. Vascular imaging included assessments of the carotid arteries or the veins of the lower limbs. The common carotid artery was imaged in B-mode for the measurement of the intima-media thickness and the bifurcation was imaged in B-mode, colour, and PW Doppler modes for the calculations of the resistance index and the quantification of stenosis (Figure 6C). The veins of the lower leg (femoral, popliteal, posterior tibial, and gastrocnemius veins) were imaged in B-mode and colour Doppler with compression being applied to the leg distal from the Doppler recording point. Thyroid investigations included transverse and longitudinal views in B-mode, colour, and PW Doppler modes and muscle examinations included the visualization of the muscle and vascular structures with both B-mode and colour.
Organs were adequately visualized, the colour and PW Doppler correctly displayed, and the diagnosis given for 97% of the examinations. In two obese patients the pancreas and gall bladder could not be visualized due to poor echogenicity. In an additional patient, edema and fat tissue prevented the proper imaging of the leg deep veins. In each of these cases the patient underwent a conventional echography examination at a radiology center.
Setup of the connections for teleoperation and the videoconference required less than 3 minutes. Each examination took an average of 17±4 minutes to complete. Using the Internet connection for teleoperation (1Mbits/s; 10 frame/s), there was about a two second lag for commands to be transmitted to the echograph and motorized probe and for the resulting modifications in the ultrasound video to be transmitted back to the expert site. The sonographer was able to accommodate for this lag after about one hour of training with the system. Additionally, the quality of the ultrasound image at the expert site was slightly lower than that on the actual echograph at the patient site; however, the images were still of good quality for medical diagnoses. On two occasions the teleoperated examination could not be performed due to a low Internet connection greatly degrading the quality of the transmitted video. Therefore, these exams were rescheduled for the following day without issue.
The teleoperated examinations performed with 15 pregnant patients in long distance sites (hospital in Ceuta n=10, and hospital in French Guyana n=5) reported similar quality of ultrasound images allowing for medical diagnoses. There was no difference in the teleoperation lag with the hospital in Ceuta using ground Internet, but the delay was increased to three seconds for examinations conducted in French Guyana (7000km from the expert sonographer) using satellite Internet. Limited testing was also conducted with the expert sonographer located away from the University Hospital (20 out of the 100 cases with the medical center) using home, mobile phone, airport, or hotel Internet connections with no detriments to the teleoperation of the echograph and probe system.
Discussion
Conclusion
Acknowledgments : The authors thank Mme. Maryannick. Porcher for her active contribution to the tele-echography examinations.
Grant Support : The present work was supported by CNES (French Space Agency), R & T grant: TOURS-2:131512-2014.
Disclosure : No conflicts of interest are declared by the authors.