Tele-operated echograph - Introduction and Methods
Echography is one of the most frequently requested forms of medical imaging requested by medical doctors after initial clinical examinations. However, even in developed countries with highly sophisticated healthcare systems, there are still wide areas where patients are required to travel more than 50 km for an ultrasound examination. Even in small cities (<10,000 people) where there are medical centers with various healthcare professionals, trained sonographers are not always present, requiring patients to travel to larger city centers for diagnostic examinations.
In most remote locations, medical professionals (paramedics, general practitioners) have no experience with clinical ultrasounds. In the minority of locations where professionals are minimally trained in the use of clinical ultrasound, they may possess the ability to visualize organs of interest but are generally unable to obtain the correct view for diagnosis without assistance from an expert sonographer. In addition, the reliability of the diagnosis from an echography examination is highly dependent on the level of training of the operator. Therefore, in small city medical centers without access to trained sonographers, the need exists for a teleoperated echography system to facilitate examinations.
Research team
- UMPS-CERCOM (Unit Med Physiol Spatiale), Faculté de Médecine, 37032 Tours, France : Philippe Arbeille (MD-PHD), Kathryn Zuj (PHD), Monica Georgescu (MD-PHD) and Joel Blouin (PHD).
- MSP (Maison de Santé Pluridisciplinaire), 37190 Richelieu, France : Arnaud Saccomandi (MD) and Elise Andre (MD).
- Dept Ostetrica i Gynecologia, Hospital Universitario, Ceuta, Espana : Jose Ruiz (MD).
- MSP (Maison de Santé Pluridisciplinaire), 37240 Ligueil France : Cedric de la Porte (MD).
- Hopital du Nord Est Guyanais, St. Laurent du Maroni, Guyane, France : Gabriel Carles (MD).
Tele-echography has been used for primary patient diagnoses in trauma or emergency situations (references 1, 2, 3) in isolated areas such as Antarctica (reference 4), and in isolated rural areas (reference 5). Several different methods of tele-echography have been investigated using different technologies such as audio-video transmission (reference 6), 3D echography (reference 7, 8), and teleoperated echographic probes (reference 9) with various degrees of success and ease of use. Regardless, the results from all of these studies confirmed the positive impact of remote echography on patient management and health outcome (reference 10).
In 2002, a first generation robotic arm to which an ultrasound probe could be attached for teleoperation through an Internet connection was developed by our group (reference 11). The system was validated in two isolated medical centers with remote abdominal, pelvic, and fetal examinations being performed successfully in 85% of the more than 110 cases (references 12, 13). The latest version of the robotic arm had a volume of 40cm by 40cm by 35cm and weighed approximately 3,5kg (reference 14). Thus, a mechanical support was necessary as the operator could not easily move the robotic arm or keep it stationary on the patient. Even using the mechanical support, the non-sonographer operator was still required to locate the probe over the appropriate acoustic window with a degree of accuracy. However, this was difficult due to the size and weight of the robot and support structure which emphasized the need for a smaller more manoeuvrable tele-operated echography system.
The objective of the current project was to develop and validate in real clinical settings a smaller, more manageable teleoperated echograph and probe system. The system would involve modifying a commercially available echograph to allow the teleoperation of the functions and settings. Also, specialized motorized probes would be developed which contain internal motors to change the orientation of the ultrasound transducer. In addition to being more manageable in clinical settings, the smaller teleoperated probe unit would be more appropriate for use in medical centers and also in other settings where there are environmental restrictions such as areas devastated after natural disasters, hazardous environments, or on the International Space Station.
Methods



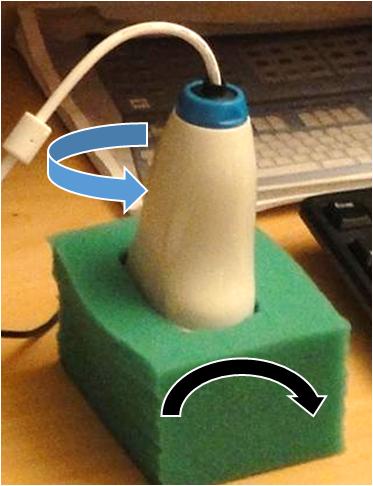
Figure 1D
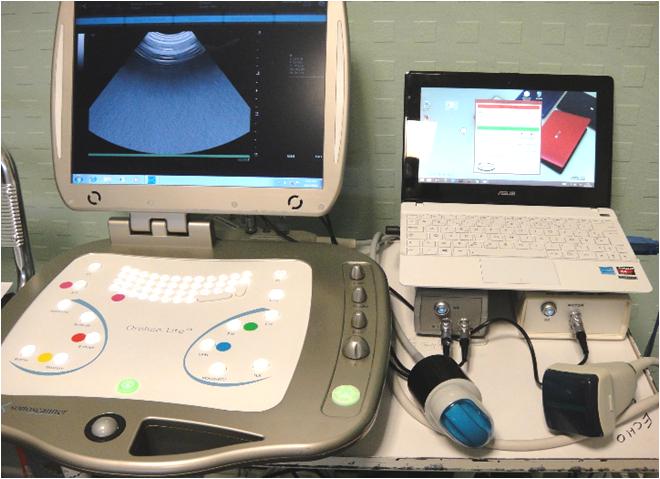

Figure 3 A : Computer for videoconferencing and the dummy probe (equipment used by the expert sonographer).
A commercially available echograph (Orcheolite, Sonoscanner, Paris, France) was modified to allow for teleoperation through an Internet connection (Teamviewer, Goppingen, Germany) (Figure 1 ; 2). At the expert site, the trained sonographer adjusted the settings (gain, depth, etc.) and functions (Doppler, colour, 3D, etc.) of the echograph using a standard keyboard (Figure 3B). Each setting or function of the echograph was identified by a letters on the keyboard, for example <F6> and <F7> increased and decreased gain where <F4> activated the PW Doppler mode. The design and weight (6kg) of the echograph was not altered; however, additional functions were added to the operation including elastography, 3D reconstruction, and radio frequency (RF) display and process.
Two specialized teleoperated probes were developed (Vermon, Tours, France) for this system which were similar to commercial 3D probes, but slightly larger and heavier (400cm3 and 430g). The first motorized probe contained a convex array transducer (3.5-7MHz) providing a wide image used for the assessment of deep organs (Figure 1A). This probe was teleoperated using one motor to tilt the transducer (+55° to -55°) and a second to rotate the transducer around the central axis (+/-180°). The second probe contained a linear array transducer (5-15MHz) used for the assessment of superficial organs (Figure 1B). In contrast to the convex probe, the linear transducer was only teleoperated using one motor for the tilt movement (+55° to -55°) as it was believed that the non-sonographer operator would be able to identify the long and shot axes of the superficial organs of interest (blood vessels, muscles). The probes were connected to the echograph using the standard probe connector and the motors were connected to an electronic module (engine pilot) external to the echograph and connected to the Internet for teleoperation (Figure 1C). Using custom software (Optimalog, St. Cyr-sur-Loire, France), movements of a dummy probe (Figure 1D) located at the expert site were mimicked by the transducer of the motorized probe at the patient site.
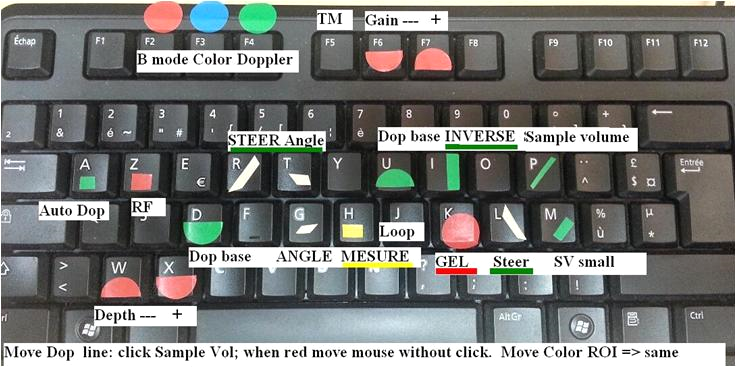
Figure 3 B : Keyboard used to control the echograph with each setting or function identified by a colour mark (equipment used by the expert sonographer).
At the patient site, a portable basic computer was used to connect the motorized probes to the Internet (Figure 2) and display the control panel for the motorized probe engines and the ambient video and sound from the expert center. An IP camera (IP AXIS camera, Paris, France) allowed the expert sonographer to communicate with the non-sonographer operator at the patient site. A switch was used to control simultaneously the Internet connection for the portable computer, the echograph, and the IP Camera.
At the expert site (Figure 3A), a basic portable computer, connected to Internet, was used to teleoperate the echograph and motorized probe and for the videoconference (IP AXIS camera, Paris, France) between the two sites. The dummy probe was connected to this computer via a USB plug. A summary schematic of the teleoperated system is presented in Figure 4.
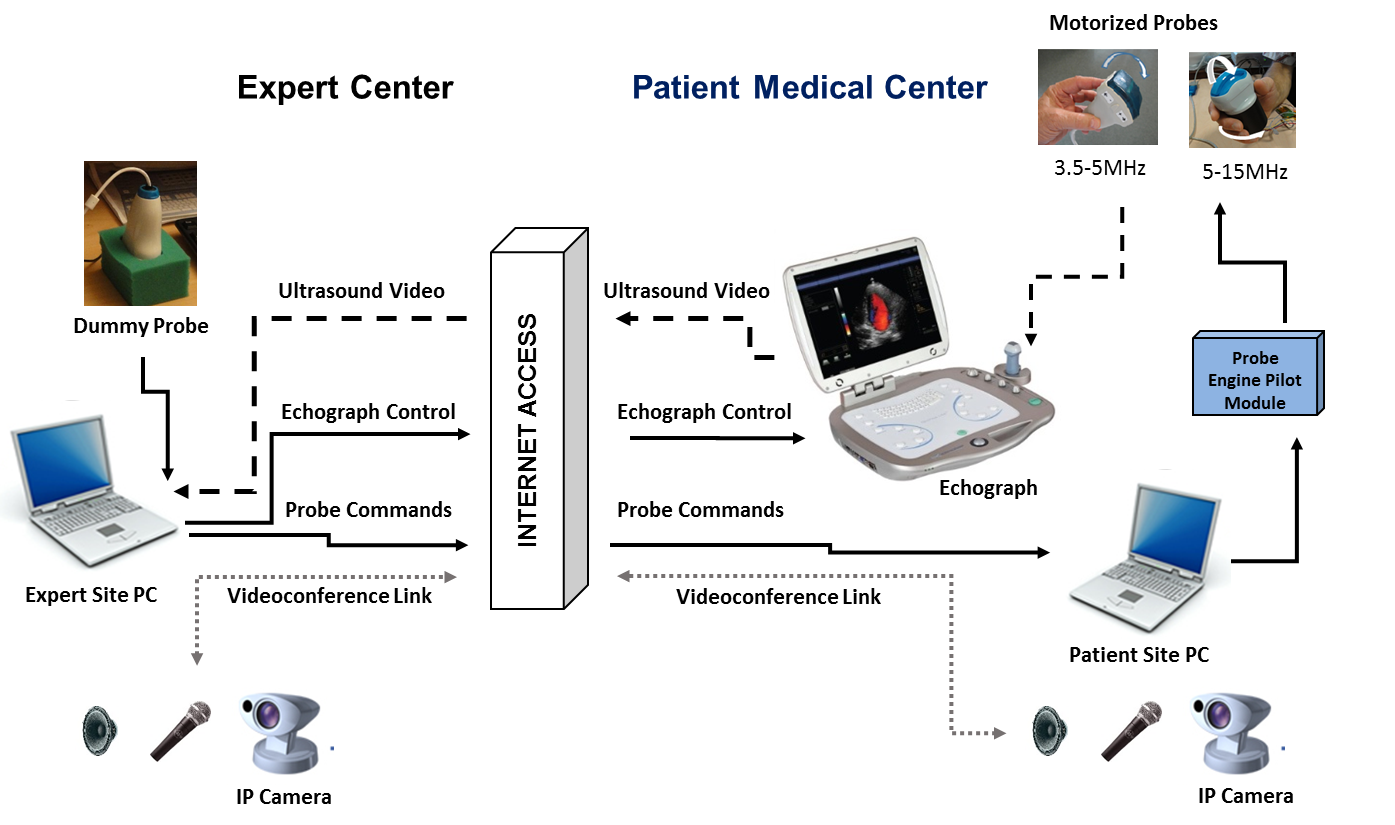
Figure 4 : Schematic summarizing the teleoperated system. Solid black arrows show the transfer of information from the expert site to the patient site to control the motorized probe transducers (Optimalog, St. Cyr-sur-Loire, France) and the echograph (Teamviewer, Goppingen, Germany). Dashed arrows show the return of the ultrasound video back to the expert site (Teamviewer). Dotted arrows show the connection for the video conference between the two sites (Teamviewer) which was accomplished using the PCs at both sites and IP cameras.
Tele-echography Procedure
The teleoperated system was used for the examination of 100 patients from two medical centres, Richelieu and Ligueil, located 50km and 60km away from the University Hospital in Tours, France and linked by ground Internet. After the initial clinical examination, the physician at the isolated medical center contacted the University Hospital to schedule the ultrasound examination within the following 24h. In some cases the examination was scheduled within 30 minutes of the physician contacting the University Hospital. Patients were recruited in the order that they arrived at the medical centers. Each patient was informed of the procedures and signed a consent form with the physician at the medical center. At the expert center, patients were identified solely by number to maintain patient confidentiality. Patient names were only introduced by the attending physician into the anonymous medical reports received from the Expert center. All protocols and procedures were approved by the University Hospital Ethics Committee (Tours, France).

To perform the teleoperated echography, the non-sonographer operator (physician or paramedic) at the patient site was required to hold and maintain the motorized probe motionless on the patient in the location indicated by the expert sonographer through the videoconference connection (Figure 5). The expert sonographer then optimized the ultrasound image by teleoperating the echograph and the motorized probe transducer. Once the appropriate view was obtained (frozen image or cineloop reviewed by the expert), video and images were saved on the computer at the expert site for inclusion in the final medical report. Video and image were also saved on the patient echograph for later review and reprocessing (measures) by the expert if need. The diagnosis was delivered to the physician verbally over the videoconference during the teleoperated examination with a follow up report, identified only by patient number, being sent via email within 30 minutes after the examination.
Additional long distance validation tests to determine the ease of use of the system were conducted with the teleoperated echograph and motorized probed unit being temporarily located in the Hospital of Ceuta (southern limit of Europe, Spain, ground Internet) and at the Apatou dispensary in the Amazonian rain forest (French Guiana, Satellite Internet) located 1800km and 7000km away from the University Hospital in Tours respectively. In both of these locations similar teleoperated echography procedures were followed, but with only a limited number of cases (10 pregnancies and 5 respectively). The physicians in each of the medical centers had previously used the robotic arm for teleoperated echography; therefore, they were asked also to evaluate the ergonomics and performance of the teleoperated echograph and motorized probes as compared to the robotic arm.
At the University Hospital, two experts who were using tele-echography in practice were asked to evaluate the time response of the motorized probe to the expert’s hand movements, the quality of the image reaching the medical center, and the use of the keyboard for adjusting echograph settings and functions. The performance of the new system was compared to that of the previous robotic arm system already medically validated (references 12, 13, 14).
Read more : Results and conclusion